
Indirect (congenital) inguinal hernias
|
An indirect (congenital) inguinal hernia is the most common, with approximately 25% being direct. Indirect hernias are also more common in males than females, which ultimately is directly related to the embryonic development of the processus vaginalis remaining open or patent rather than regressing and closing off its connection and opening between the abdominal cavity once the testes have migrated. However, indirect hernias in females are more common than direct, resulting from the deep inguinal ring remaining patent.
|
Protrusion of the peritoneal sac occurs through the deep inguinal ring, lateral to the inferior epigastric vessels and passing into the inguinal canal, seen in Figure 19 (Drake et al. 2010). In males this peritoneal sac, formed by the processus vaginalis and the fascial coverings of the spermatic cord, can often pass through the superficial inguinal ring, however this is dependent on whether the entire processus vaginalis remains. In females a peritoneal protrusion can also extend into the labia majora, which is termed the Canal of Nuck. In both cases the protrusion of the peritoneal sac acquires the three coverings of fascia derived from the anterior abdominal wall.
|
Scroll over both the labels and the structures in the image below to highlight them and/or reveal where they are located. By clicking on various structures descriptions will appear under some areas.
Figure 28. Indirect inguinal hernia, adapted from (Drake et al. 2010: p.288).
There are three types of indirect (congenital) inguinal hernias, classified on their anatomical relationships:
Bubonocele:
Hernia located within the inguinal canal and has not protruded through the superficial inguinal ring
Funicular:
The processus vaginalis is closed at it distal end, superior to the epididymis with the content of the sac separate to the testis
Complete (or scrotal):
The hernia sac descends to the scrotum where it is continuous with the tunica vaginalis and subsequently the processes vaginalis is patent.
Hernia located within the inguinal canal and has not protruded through the superficial inguinal ring
Funicular:
The processus vaginalis is closed at it distal end, superior to the epididymis with the content of the sac separate to the testis
Complete (or scrotal):
The hernia sac descends to the scrotum where it is continuous with the tunica vaginalis and subsequently the processes vaginalis is patent.
Direct (acquired) inguinal hernias
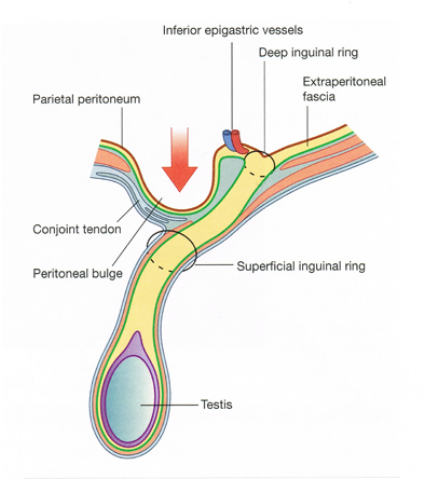 Figure 20. Direct inguinal hernia (Drake et al. 2010: p.289).
Figure 20. Direct inguinal hernia (Drake et al. 2010: p.289).
A direct inguinal hernia is described as a protrusion of the peritoneum through a weakened posterior abdominal wall of the transversalis fascia and into the medial region of the inguinal canal, seen in Figure 20 (Drake et al. 2010). The peritoneal sac protrudes medially in relation to the inferior epigastric vessels and within the inguinal triangle, seen in Figure 21 (Drake et al. 2010), also known as Hesselbach's triangle. The boundaries of the inguinal triangle include:
Medially: Lateral margin of the rectus sheath
Laterally: Inferior epigastric vessels
Inferiorly: Inguinal ligament
Subsequently a direct inguinal hernia does not protrude through the entire length of the inguinal canal but can protrude through the superficial inguinal ring, acquiring the external spermatic fascia and very rarely extending into the scrotum lateral to the spermatic cord.
Medially: Lateral margin of the rectus sheath
Laterally: Inferior epigastric vessels
Inferiorly: Inguinal ligament
Subsequently a direct inguinal hernia does not protrude through the entire length of the inguinal canal but can protrude through the superficial inguinal ring, acquiring the external spermatic fascia and very rarely extending into the scrotum lateral to the spermatic cord.
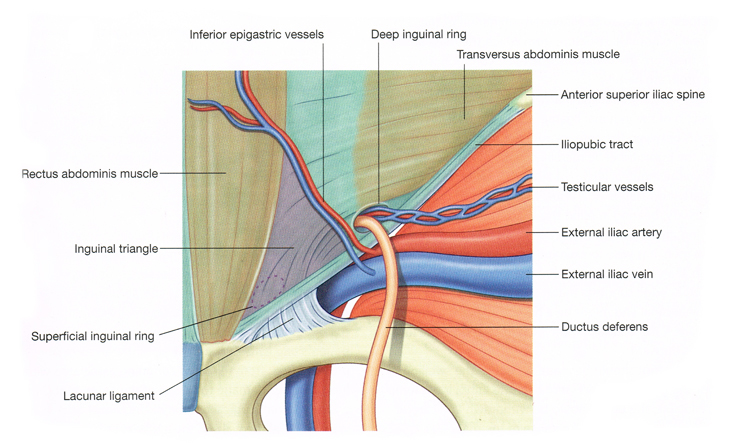
Figure 21. Right inguinal triangle - Internal view (Drake et al. 2010: p. 289).
Sliding hernia:
In 3% of inguinal hernia cases this variant can be observed. It occurs when part of the retroperitoneal fat and/or organs, which can be the uterus, uterine tubes, ovaries, bladder, ureters on both sides or the caecum, ascending colon or appendix on the right and the sigmoid colon on the left, protrudes through an abdominal wall opening with or without the adjacent peritoneal sac. Both the viscera and the peritoneal sac lie within the inguinal canal. These herinas can be either indirect or direct and occur most commonly in males.
In 3% of inguinal hernia cases this variant can be observed. It occurs when part of the retroperitoneal fat and/or organs, which can be the uterus, uterine tubes, ovaries, bladder, ureters on both sides or the caecum, ascending colon or appendix on the right and the sigmoid colon on the left, protrudes through an abdominal wall opening with or without the adjacent peritoneal sac. Both the viscera and the peritoneal sac lie within the inguinal canal. These herinas can be either indirect or direct and occur most commonly in males.
