
Laparoscopic Repair
Laparoscopic repairs require several small incisions, are done under general anesthesia and require more time compared with the open repair technique. Those surgeons experienced in it only carry out this technique.
|
The basic principle of these repairs is the placement of the mesh in the preperitoneal space, seen in Figure 31 (Drake et al. 2010). The methods of repair can be divided into groups based on either accessing the abdomen or without entering the abdominal cavity, with the most commonly used being the transabdominal preperitoneal repair (TAPP) and the total extraperitoneal repair (TEP). The TAPP approach repairs the defect from within the abdomen, accessing the preperitoneal space through an incision in the peritoneum where a polypropylene mesh is attached using tacks. The TEP approach repairs the defect from the extraperitoneal space with non-absorbable mesh using tacks.
|
If a bilateral hernia is present this laparoscopic technique is advised because it allows for both hernias to be repaired in this one operation. When undergoing laparoscopic repair for a unilateral hernia, reduced pain and earlier return-to-work has been reported compared with open repairs, although complications are more common during laparoscopic surgery. However, both open repairs and laparoscopic repairs have been found to have excellent results when the hernia is uncomplicated and unilateral and is not recurrent.
With both the TAPP and TEP approaches the patient is placed in the supine position and general anesthesia is administered. |
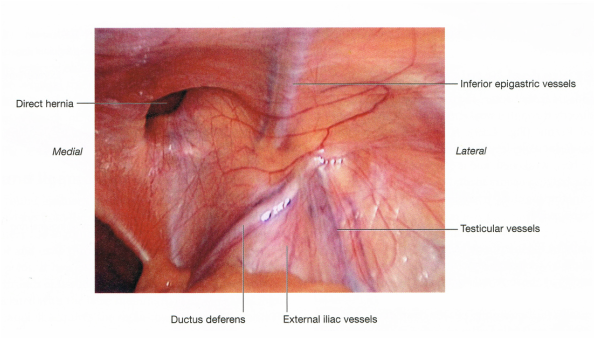
Figure 31. Right inguinal triangle, laparoscopic view showing the parietal peritoneum still covering the area (Drake et al. 2010: p. 290).
The TAPP Approach:
The TAPP approach accesses the preperitoneal space through three incisions in the peritoneum and three trocars are inserted along with a laparoscope to inspect the groin anatomy, with the inferior epigastric vessels, the spermatic vessels, and the vas deferens identified. The myopectineal orifice is dissected free of peritoneum and preperitoneal fat and the peritoneum is bluntly dissected off transversus abdominus and transversalis fascia until the pubic bone, Cooper’s ligament, and iliopubic tract can be seen and the inguinal floor is exposed to reveal either the direct or indirect hernia, with an indirect (congenital) hernial sac usually found on the antero-lateral side of the cord and can be dissected whilst ensuring minimal trauma to the vas deferens and the spermatic vessels. If a direct (acquired) hernia is present this can be reduced. Mesh is used to overlap the myopectineal orifice in both a direct or indirect inguinal hernia, seen in Figure 32 (Carter and Duh, 2011) and fixed either with glue, sutures or a sutureless repair is carried out, fixing it to the iliopubic tract, and Cooper’s ligament.
The TAPP approach accesses the preperitoneal space through three incisions in the peritoneum and three trocars are inserted along with a laparoscope to inspect the groin anatomy, with the inferior epigastric vessels, the spermatic vessels, and the vas deferens identified. The myopectineal orifice is dissected free of peritoneum and preperitoneal fat and the peritoneum is bluntly dissected off transversus abdominus and transversalis fascia until the pubic bone, Cooper’s ligament, and iliopubic tract can be seen and the inguinal floor is exposed to reveal either the direct or indirect hernia, with an indirect (congenital) hernial sac usually found on the antero-lateral side of the cord and can be dissected whilst ensuring minimal trauma to the vas deferens and the spermatic vessels. If a direct (acquired) hernia is present this can be reduced. Mesh is used to overlap the myopectineal orifice in both a direct or indirect inguinal hernia, seen in Figure 32 (Carter and Duh, 2011) and fixed either with glue, sutures or a sutureless repair is carried out, fixing it to the iliopubic tract, and Cooper’s ligament.
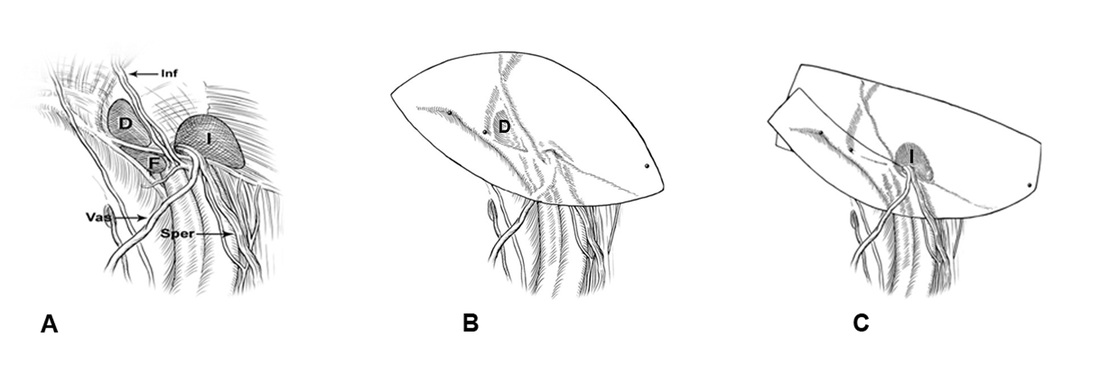
Figure 32. A. Right groin anatomy. The intersection of these three structures forms the ‘‘Mercedes-Benz’’ sign. D direct hernia, F femoral hernia, I indirect hernia, Inf inferior epigastric vessels, Sper spermatic vessels, Vas vas deferens. B. Mesh repair of right-sided direct hernia. C. Mesh repair of right-sided indirect hernia, adapted from (Carter and Duh, 2011: p. 1521-1523).
The TEP Approach:
For a TEP approach the repair is similar to that carried out by the TAPP but the defect is approached from the extraperitoneal space and a non-absorbable mesh is used. Whether the approach is a TAPP or a TEP depends on the preference of the surgeon with the major difference between the two approaches being the time it takes to learn them with a far higher learning curve for the TEP compared with the TAPP.
For a TEP approach the repair is similar to that carried out by the TAPP but the defect is approached from the extraperitoneal space and a non-absorbable mesh is used. Whether the approach is a TAPP or a TEP depends on the preference of the surgeon with the major difference between the two approaches being the time it takes to learn them with a far higher learning curve for the TEP compared with the TAPP.
The technique used to repair the inguinal hernia; open repair or laparoscopic depends on whether the hernia is direct or indirect, its size and whether it is incarcerated or strangulated and either a recurrent or primary hernia. The patients age must also be taken into account. The anterior versus preperitoneal approach, the fixation of the mesh in front of the trasversalis fascia or in the preperitoneal space and whether the fixation is via a suture or is sutureless depends on the preference of the surgeon.
