
Symptoms of Inguinal Hernias
The patient can present with a number of symptoms, which can include a protrusion or lump in the groin region and in males can include an enlargement of the scrotum, with mild to moderate discomfort that increases through activity such as lifting a heavy object or through urination or defecation. With larger hernias patients may present with a dragging sensation and pain.
If the hernia is strangulated the patient may present with a fever, vomiting and/or nausea, rapid heart rate, pain that quickly intensifies, loss of appetite and a darkened hernial protrusion.
Diagnosis of Inguinal Hernias
Diagnosis can be made firstly by looking at the patients medical and family history and via a physical examination when the patient is both standing and seated. With the patient standing they are asked to cough whilst observing any noticeable transient protrusion or lump present, which can be palpable. Any asymmetry can also be accessed to determine whether a bilateral hernia present. With the patient in the supine position the abdominal region should be examined to access further for any protrusion or lump. However, if the hernia is reduced it may not be possible to observe. If a protrusion is present and noticeable the hernia may be reducible. To determine this the patient is asked to recline, which may reduce the hernia but it may require manual replacement by applying pressure over the deep inguinal ring whilst asking the patient to cough. If this is successful it is referred to as a reducible hernia.
|
If adhesions have formed the hernia may not be reducible and can be classified as irreducible or incarcerated which can lead to a strangulated inguinal hernia. If this is suspected and there have been episodes of prolonged pain and tenderness surgery is recommended with emergency surgery advised for a suspected strangulated hernia to restore blood supply to the trapped tissue.
|
If a protrusion cannot be felt during a physical exam, the swelling cannot be accurately or easily diagnosed or if an incarcerated or strangulated inguinal hernia is suspected further analysis can be made via an ultrasound examination, an abdominal X-ray, computerized tomography (CT) scans a herniography and an MRI scan, seen in Figure 22 (Drake et al. 2010).
|

Figure 22. Right indirect inguinal hernia. T2, fat saturated, weighted magnetic resonance image in the coronal plane of a male groin (Drake et al. 2010: p.291).
During a physical examination the index finger can be placed onto the skin of the upper scrotum and by invaginating the skin in this region the superficial inguinal ring, seen in Figure 23 (Moore et al. 2010), which is lateral to the pubic tubercle can be palpated by advancing the finger in a superolateral direction along the spermatic cord. When the patient is asked to cough a sudden protrusion can be felt if a hernia is present. However, this process is an uncomfortable procedure for the patient and can be further accessed by locating the deep inguinal ring, which can be found midway between the anterior superior iliac spine and the upper margin of the pubic bone. This examination can determine whether an inguinal hernia is present but it cannot determine whether the inguinal hernia is either indirect or direct due to both hernias exiting through the superficial inguinal ring.
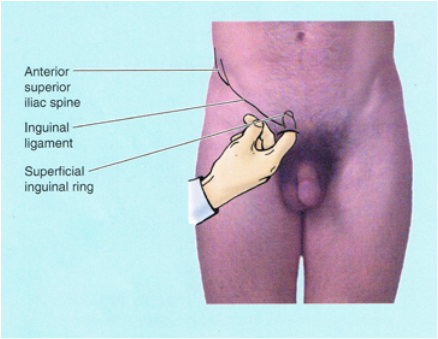
Figure 23. Palpation of the superficial inguinal ring, for both indirect and direct inguinal hernias (Moore et al. 2010: p. 214).
Diagnosis of Indirect (congenital) Inguinal Hernias:
Indirect (congenital) inguinal hernias can be diagnosed by palpating the inguinal rings. Palpation of the deep inguinal ring, by placing the finger on the anterior abdominal wall, a skin depression can be felt superior to the inguinal ligament. If a hernia is present it may be reducible, which can be determined by trying to reduce it. If a protrusion is not present the patient is asked to cough to confirm if one becomes palpable and whether a hernia is present or not.
Indirect (congenital) inguinal hernias can be diagnosed by palpating the inguinal rings. Palpation of the deep inguinal ring, by placing the finger on the anterior abdominal wall, a skin depression can be felt superior to the inguinal ligament. If a hernia is present it may be reducible, which can be determined by trying to reduce it. If a protrusion is not present the patient is asked to cough to confirm if one becomes palpable and whether a hernia is present or not.
Diagnosis of Direct (acquired) Inguinal Hernias:
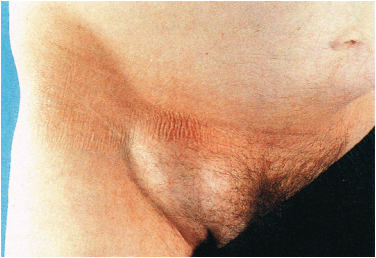 Figure 24. Right direct inguinal hernia (Douglas et al. 2009: p.205).
Figure 24. Right direct inguinal hernia (Douglas et al. 2009: p.205).
Direct (acquired) inguinal hernias, seen in Figure 24 (Douglas et al. 2009) can be diagnosed by placing the index finger over the inguinal triangle and palpating this region, whilst asking the patient to cough. If a hernia is present a sudden protrusion will be felt.
Placing the finger in the superficial inguinal ring, as described earlier can determine whether a direct and an indirect inguinal hernia is present but it can not differentiate between the two.
Differential Diagnosis
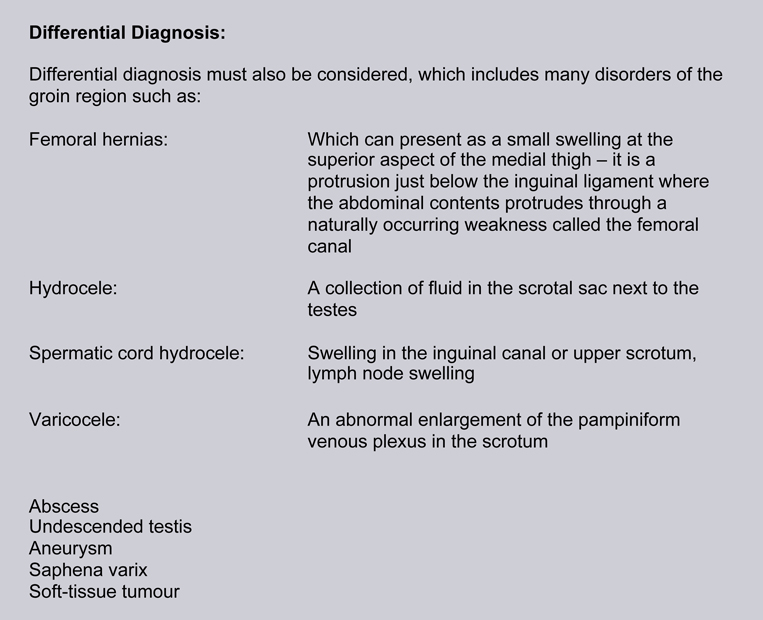
Examples of two of these disorders associated with indirect (congenital) inguinal hernias are a hydrocele of the testes and a hydrocele of the cord, seen in Figure 25 (Moore et al. 2010).
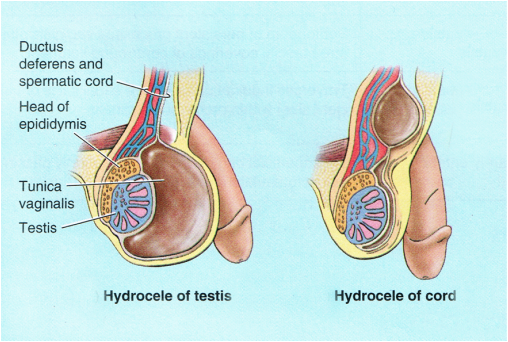
Figure 25. Two disorders associated with an indirect inguinal hernia, a hydrocele of the testes and a hydrocele of the cord, adapted from (Moore et al. 2010: p. 214).
