
Hernioplasty
These repairs were introduced in the 1960s and are based on synthetic biomaterials to repair the defect, which have subsequently decreased the risk of complications and reduced hernia reoccurrence rates. However, one such common and most popular synthetic material used is a polypropylene mesh but this also has a tendency to shrink up to 30% over time.
These mesh based repairs replace or reinforce the transversalis fascia placing the mesh over the defect in the myopectineal orifice and can be further grouped into anterior (focusing on the superior aspect of the inguinal canal) and includes the Lichtenstein tension-free repair, posterior (focusing on the preperitoneal space), which includes the Kugel and Plug repairs and mixed approaches, consisting of both an onlay and underlay mesh, which includes the Prolene Hernia System. All of these approaches shall be discussed below.
These mesh based repairs replace or reinforce the transversalis fascia placing the mesh over the defect in the myopectineal orifice and can be further grouped into anterior (focusing on the superior aspect of the inguinal canal) and includes the Lichtenstein tension-free repair, posterior (focusing on the preperitoneal space), which includes the Kugel and Plug repairs and mixed approaches, consisting of both an onlay and underlay mesh, which includes the Prolene Hernia System. All of these approaches shall be discussed below.
Anterior Approach
Lichtenstein tension-free repair:
|
This is an anterior mesh based approach and one of the most commonly used during inguinal hernia surgery. This repair is an example of a hernioplasty where reinforcement is applied to the posterior wall of the inguinal canal with a synthetic mesh, seen in Figure 28 (Kingsnorth and LeBlanc, 2003), rather than repairing the posterior wall directly when using the Bassini and Shouldice methods in a herniorrhaphy. Lichtenstein tension-free repairs can be performed using local anesthesia with low recurrence rates of 1% reported, however shrinkage and migration of the mesh has also been reported but complications are minimal.
|
The inguinal canal is exposed via an incision in the aponeurosis of external oblique and any indirect and direct hernia is reduced. The polypropylene mesh is sutured using a continuous absorbable monofilament suture sewn to the conjoint tendon and an nonabsorbable suture on the inguinal ligament, reinforcing the floor and a slit is made in the mesh to accommodate the cord structures. Laterally the mesh covers the deep inguinal ring and medially it overlaps the pubic tubercle. The external oblique aponeurosis is closed over the cord structures and the repair is complete.
|
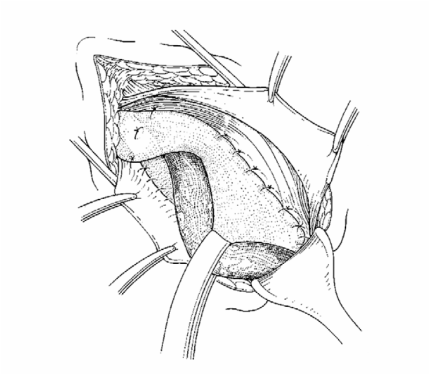
Figure 28. The flat patch Lichtenstein operation
(Kingsnorth and LeBlanc, 2003: p.1563).
Trabucco repair:
This is similar to the Lichtenstein tension-free repair but it is a tension-free sutureless repair within the posterior wall of the inguinal canal. It uses a flat rigid pre-shaped memory mesh and can be used for primary inguinal hernias.
This is similar to the Lichtenstein tension-free repair but it is a tension-free sutureless repair within the posterior wall of the inguinal canal. It uses a flat rigid pre-shaped memory mesh and can be used for primary inguinal hernias.
Posterior approach
Plug techniques:
These repairs involve a triangular or cone polypropylene mesh to repair the defect in the posterior inguinal wall specifically with the insertion of the mesh through the defect in the myopectineal orifice. Due to its semi-rigid shape, postoperative pain has reported in up to 8% of patients along with shrinkage and migration of the mesh.
These repairs involve a triangular or cone polypropylene mesh to repair the defect in the posterior inguinal wall specifically with the insertion of the mesh through the defect in the myopectineal orifice. Due to its semi-rigid shape, postoperative pain has reported in up to 8% of patients along with shrinkage and migration of the mesh.
|
Gilbert umbrella plug:
This is a sutureless repair, modified from the Litchenstein tension-free repair and is a posterior repair via an anterior approach. This repair uses a triangular polypropylene mesh to repair the defect and is approached through the deep inguinal ring, to enter the preperitoneal space and plug the defect in the posterior inguinal wall. |
Plug and patch:
The plug-and-patch method repairs the defect in the deep inguinal ring or inguinal canal floor, reinforcing it and consists of the placement of a polypropylene mesh cone-shaped plug at this defect, which can be supplemented with a small flat mesh if required. |
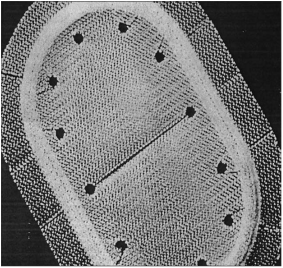 Figure 29. The Kugel Patch (Awad and Fagan, 2004: p. 13S).
Figure 29. The Kugel Patch (Awad and Fagan, 2004: p. 13S).
Kugel patch:
The Kugel patch repair consists of a bilayered polypropylene mesh, seen in Figure 29 (Awad and Fagan, 2004) and is self-expanding with a memory recoil ring, which helps to maintains its shape. A smaller incision is made (3-4cm) and it is placed anteriorly within the preperitoneal space deep to the myopectineal defect.
This repair is not recommended for recurrent hernias.
The Kugel patch repair consists of a bilayered polypropylene mesh, seen in Figure 29 (Awad and Fagan, 2004) and is self-expanding with a memory recoil ring, which helps to maintains its shape. A smaller incision is made (3-4cm) and it is placed anteriorly within the preperitoneal space deep to the myopectineal defect.
This repair is not recommended for recurrent hernias.
mixed approach
The Prolene Hernia System:
This repair is recommended for both direct and indirect hernias. It consists of both an underlay and onlay mesh with a connector, seen in Figure 30 (Awad and Fagan, 2004). The underlay is placed in the preperitoneal space and the onlay is placed in the subfascial space and sutured to the inguinal ligament and conjoint tendon, similar to that in the Lichtenstein tension-free repair. The connector attaches the underlay to the onlay at the defect and helps to maintain its position and prevent migration of the mesh.
This system combines the anterior repair with the preperitoneal placement of the mesh and has shown a very low rate of recurrence.
This repair is recommended for both direct and indirect hernias. It consists of both an underlay and onlay mesh with a connector, seen in Figure 30 (Awad and Fagan, 2004). The underlay is placed in the preperitoneal space and the onlay is placed in the subfascial space and sutured to the inguinal ligament and conjoint tendon, similar to that in the Lichtenstein tension-free repair. The connector attaches the underlay to the onlay at the defect and helps to maintain its position and prevent migration of the mesh.
This system combines the anterior repair with the preperitoneal placement of the mesh and has shown a very low rate of recurrence.
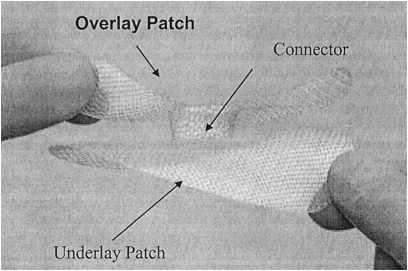
Figure 30. The Prolene Hernia System (Awad and Fagan, 2004: p. 14S).
